A 45 year old man, presented with history of worsening breathlessness and generalised edema since 10 days
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Here is a case i have seen:
The patient's first recall of medical problems began well over an year ago, when he first noticed an indolent breathlessness, which he felt was unusual to his daily activity - auto rickshaw driving. He remembers that his breathlessness was associated with heavy palpitations and mild sweating.The patient cannot recall having any problems until 8 months ago, he had to wake up from his sleep, breathless and a need for fresh air. Even this episode was associated with similar palpitations and a more profuse sweating.
The patient reported that 6 months ago, he started to notice frothy urine and an occasional blood discharge in urine. He denies a history of decreased urine output back then, nocturia, pyuria or red casts in his urine. He also denied pedal edema and facial puffiness at that point. These concerns have been troublesome to him since then. With an insidiously progressing dyspnea and palpitations (on our questioning), the patient started developing pedal edema and facial edema since the last 2 months. On pressing further, he reported that both pedal edema and facial started at the same time. He also started developing adnominal distension for the last 1 month. At this point he started having decreased urine output and nocturia. He denies having any LUTS. He denies vomiting, diarrhea or consistent night sweats at any point. He reported a low grade fever since 2 months. He also reported a loss of appetite since 2 months but so weight loss. He denies constipation, afternoon fatigue, jaudice, altered taste, abnormal sleeping habits or syncope.
The patient reports that in the last 10 days, his dyspnea and edema increased to incapacitating levels, with dyspnea on walking a few steps and an anasarca so severe that he couldn't open his eyes in the morning.
The patient and his family have a past history of a fever and joint pains syndrome 1 year ago which subsided within a week.
He does not have any other relevant past history. He is a self confessed alcoholic and an avid smoker. The wife says he is underplaying his alcoholism and she confides that he sometimes goes day on end with alcohol intake only and no food whatsoever. He smokes about 10 'Bristol' cigarettes a day and he denies having illicit sexual relations.
He also has a past history of exploratory laparotomy for ? Hollow Viscus Perforation 6 years ago. The scar is now hypertrophic.
After a lengthy interview, the patient settles in well and develops, what we felt, a sense of trust and understanding in our methods.
On examination:
Temp - 98F
PR - 87
RR - 18
BP - 100/60
SpO2 - 99
GRBS - 111
Positive Findings -
Pallor, clubbing- parrot beak appearance
Icterus, bilateral pedal edema.






CVS:
Raised JVP (video above) Palpable P2, RV Pulsations, Apex Normal
Palpable pulsation in left lower sternal region
Apex beat in 5th intercoastal space(10cm from sternum)
Auscultation: S1S2 heard
Pulmonary area, Tricuspid area and left sternal border S3 heard.
Audicor:


Perabdomen:
Distended, left palpable mass near umbilicus.
Bowel sounds +
Palpable Non Tender Liver with span of 15.5cm in midclavicular line. No splenomegaly or dilated abdominal veins.
Hepatic veins on USG 1cm (>7mm abnormal)
20 x 1.5 cm hypertrophic scar noted in midline (images above)
Pitting type of pedal edema and mild scrotal edema.
Diagnosis :
1) HFPeF with moderate PAH
2)Alcoholic Hepatitis with AKI with
Congestive hepatopathy.
Investigations:
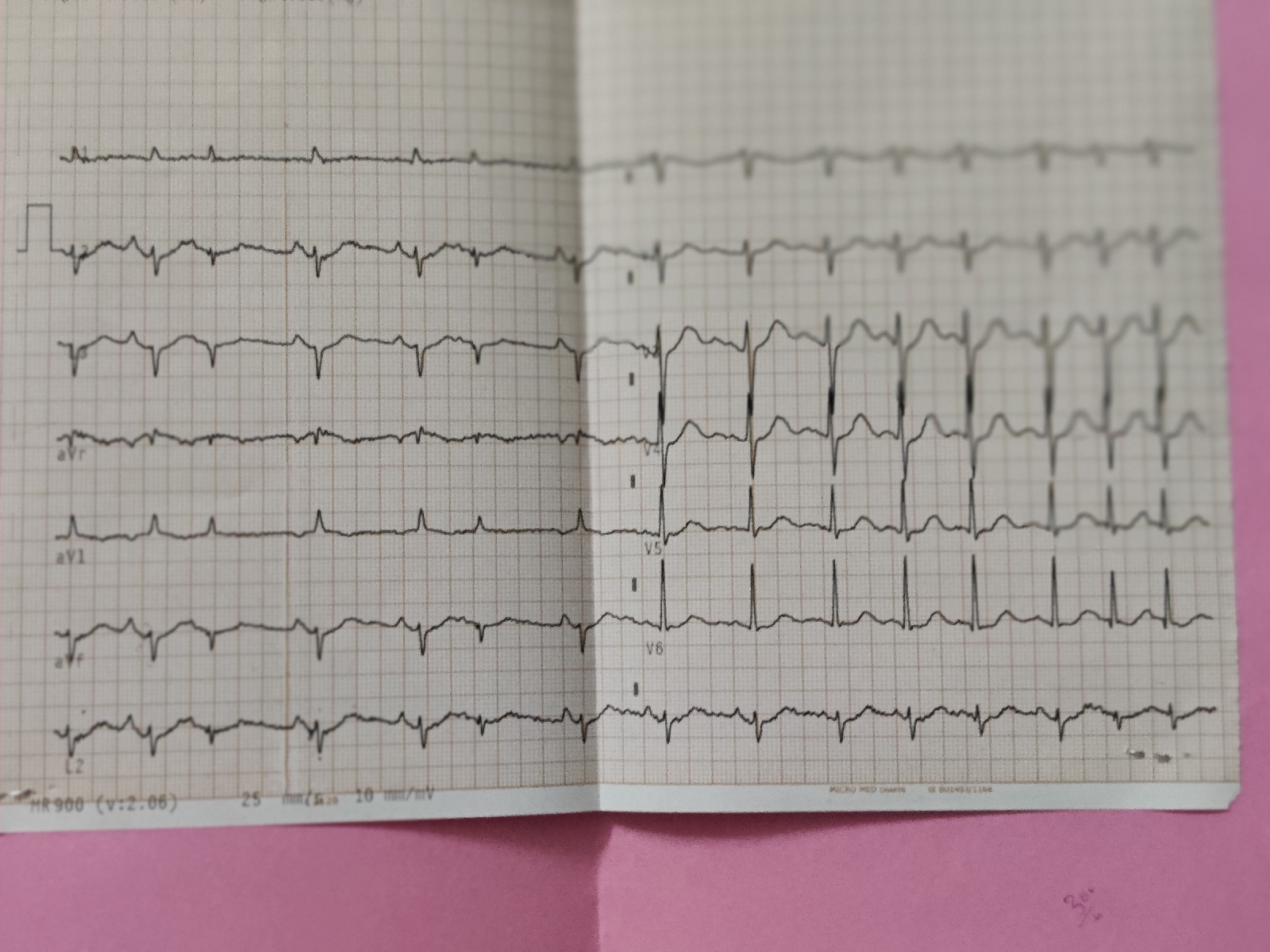
ECG


2d echo:



Review USG - mass per Abdomen:
Divarication of recti noted.
Day 1:
Salt restriction <2 gm/day
Fluid restriction < 1L/day
Inj.Thiamine 1 amp in 100ml NS IV OD
Inj.Lasix 40 MG IV BD
Day 2:
Salt restriction <2 gm/day
Fluid restriction < 1L/day
Inj.Thiamine 1 amp in 100ml NS IV TID
Inj.Lasix 40 MG IV BD
Inj.Pantop 40 mg IV OD.
Day 3:
Same treatment as above

Comments
Post a Comment