55 year man with Recurrent Focal seizures
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Here is a case i have seen:
Today at 9am while he was sitting in his chair, drinking tea , he suddenly started complaining that he couldn’t move his right upper limb few minutes later he developed a sudden onset, tonic clonic seizures involving his right upper limb and lower limb lasting for 2 minutes following which he had another 8 episodes of focal seizures involving his right upper limb and right lower limb with a 2 minutes of gap between each episode. During these episodes he had uprolling of eyes and wasn’t followed by froth discharge from mouth or tongue bite or any involuntary micturation. He was in postictal confusion lasting for 40 minutes. He was immediately taken to a nearby hospital where he was given certain medications ( not documented) , he apparently had two more episodes of GTCS during his hospital stay. After which he was brought to our hospital.
On presentation to us his GCS was 15, and he was drowsy His
PR was 150bpm
BP 170/90mmhg
Temp 99.8F
Saturations at 85%
GRBS 325mg/dl
Clubbing +
CNS - bilateral pupils reacting to light






 Impression:
Impression:

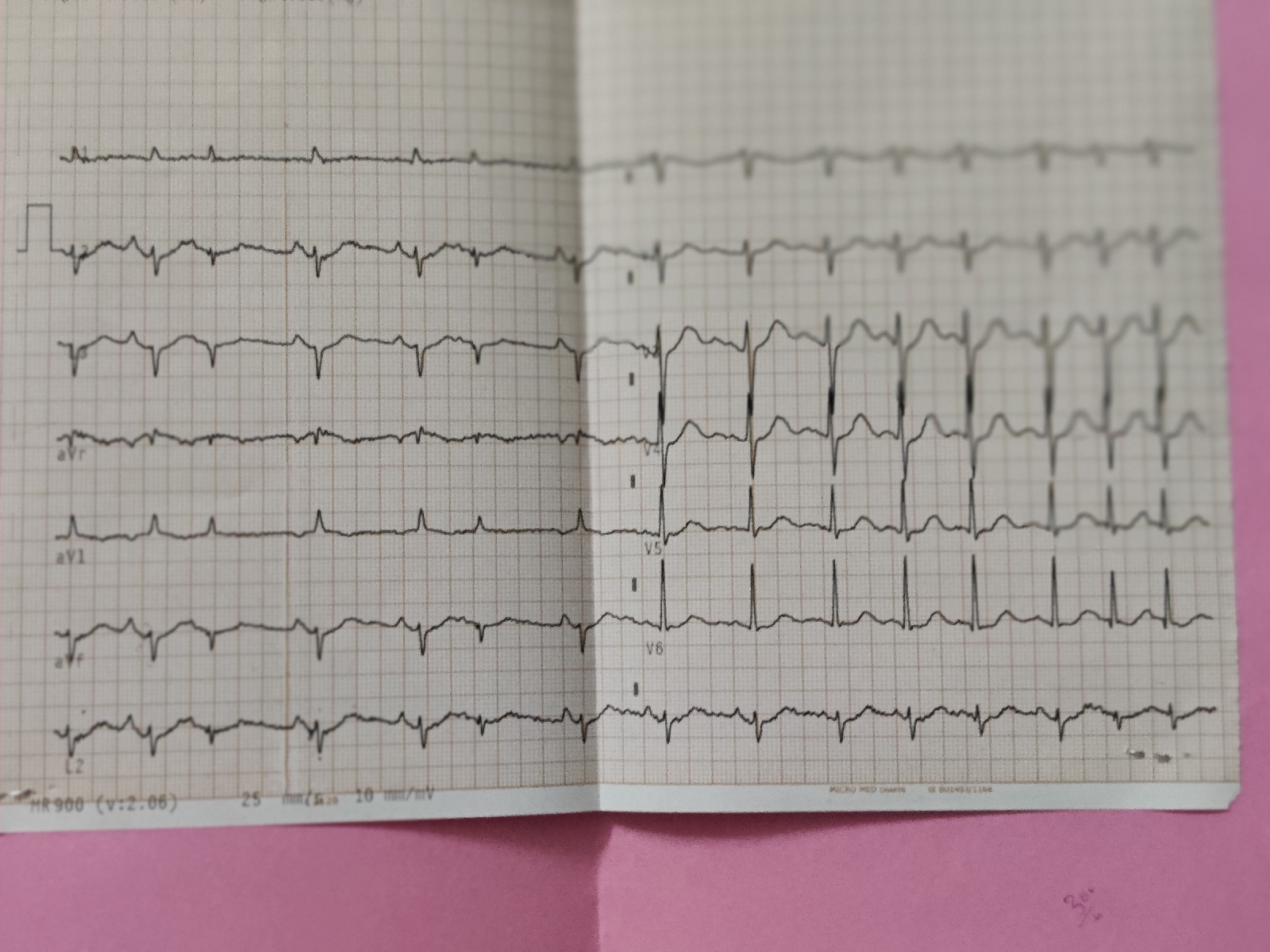
ECG:






 Day4/12:
Day4/12:
 Day 5/12:
Day 5/12:




 At 3am he has 1episode of seizures lasting for 1minute.
At 3am he has 1episode of seizures lasting for 1minute.




Power Right. Left
UL. 0/5. 3/5
LL -4/5. +4/5
Reflexes. Right. Left
B. - 2+
T. - 2+
S. - 2+
K. 2+. 2+
A. - -
Plantars - withdrawal bilaterally
Respiratory system - Bilateral inspiratory crepts in all areas, Right > Left
CVS - muffled S1,S2
P/A - non tender
Soft
Bowel sounds +
He had to be sent to another hospital for a CT or MRI brain as it’s not working in the hospital
CT Brain:
Impression:

MRI Brain:
EEG:
Abnormal EEG record- suggestive of right temporal epileptogenic focus.
Day28/11:
Day 29/11:
Day 30/11:
Day 1/12:
Day 2/12:

Day 3/12:
2D ECHO:
Seizure episodes graphical representation:
Investigations:
Day 1
Day 2
Day 3:
On day 3 he has 1 episode of focal seizures lasting for an hour.
Diagnosis:1) Recurrent Focal seizures(secondary to CVA)
2)Right hemiparesis with acute ischemic infarct in left fronto parietal area
3)Right multiple chronic infarcts
4)Cardioembolic stroke
5)K/C/O type 2 diabetes mellitus
6)NSTEMI in Anteroseptal leads
Treatment:
Day 1:
Oxygen supplementation@ 2-4 L/min
Inj.Levipil 1gm/IV in 100ml NS
Isosorbitate 5mg sublingual
Day 2:
Propped up posture
Oxygen inhalation with 4 litres of oxygen( maintain spO2 >90%
Nebulisation with Duolin 6th HRLY
Mucomist 6th HRLY
Budecort 12 HRLY
Inj.Levipil 500 mg IV BD
Inj.Lorazepam 2 ml IV SOS
Inj.Thiamine 1 amp in 100ml NS /TID
Tab. Ecosprin 75 mg PO HIS
Tab.Atorvas 10 mg PO OD
Inj. Mannitol 100gm IV TID
Inj.PAN 40 mg IV OD BBF
Inj. HUMAN MIXTARD s/c
Tab.Metformin 500mg ODA
Inform SOS
Day 3:
Propped up posture
Oxygen inhalation with 4 litres of oxygen( maintain spO2 >90%
Nebulisation with Duolin 6th HRLY
Mucomist 6th HRLY
Budecort 12 HRLY
Inj.Levipil 500 mg IV BD
Inj.Lorazepam 2 ml IV SOS
Inj.Thiamine 1 amp in 100ml NS /TID
Tab.Carbamazepine 200mg PO BD
Inj.ENOXOPARIN 30 mg IV STAT followed by Inj. ENOXAPARIN 60 mg /sc/BD
Tab. Ecosprin 75 mg PO HIS
Tab.Atorvas 10 mg PO OD
Inj. Mannitol 100gm IV TID
Inj.PAN 40 mg IV OD BBF
Inj. HUMAN MIXTARD s/c
Tab.Metformin 500mg ODA
Inform SOS
Day4:
Head end elevation
Oxygen supplementation if spO2<90%
Nebulisation with Duolin 6th HRLY
Mucomist 6th HRLY
Budecort 12 HRLY
Inj.Levipil 500 mg IV BD
Inj.Lorazepam 2 ml IV SOS
Inj.Thiamine 1 amp in 100ml NS /TID
Tab.Carbamazepine 200mg PO BD
Tab. Ecosprin 75 mg PO HIS
Tab.Atorvas 10 mg PO OD
Inj. Mannitol 100gm IV TID
Inj.PAN 40 mg IV OD BBF
Inj.ENOXAPARIN 60mg/sc/BD for 5 days
Inj. HUMAN MIXTARD s/c
Tab.Metformin 500mg ODA
Inform SOS
Day 4 soap notes:
No seizure episode since last night
PR - 72 bpm
BP- 120/80mmhg
RR- 21 Cpm
SPO2 - 92 on RA
Afebrile
Cvs - S1,S2
Lungs - inspiratory crepts in bilateral IAA, ISA region
CNS -
Power improved comparitively
Right. Left
UL. -4/5. +4/5
LL. -4/5. +4/5
P/A - soft
Non tender
Bowel sounds +
A - Focal seizures secondary to ? Right frontoparietal ischaemic infarcts
P-tab.carbamazepine with hold
Tab.levipil 500mg bd

Comments
Post a Comment